Spinulate demodicosis.: Primary human demodicosis depicting discrete, fine, whitish, partly yellowish, keratotic, spiky scaly changes involving sebaceous hair follicles in the background of faint erythema:

Papulopustular demodicosis. (a) Primary human demodicosis characterized by a typical protracting course involving the forehead of a 46-year-old man with agminated follicle-bound lesions in an irregular shape. (b) Microscopic examination of skin scrapings revealed more than 5 mites per cm2:

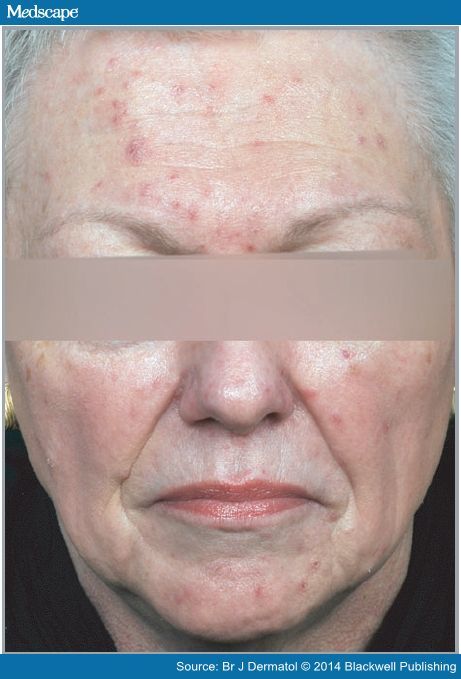
Papulopustular demodicosis. Primary human demodicosis displaying disseminate involvement of the face of a 64-year-old woman with mild keratotic inflammatory papules of different sizes in an asymmetric distribution:
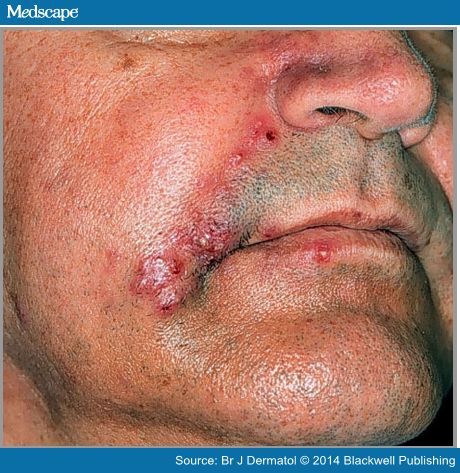
Nodulocystic demodicosis. Primary human demodicosis with intense inflammatory reaction including pus and
suppurative succulent changes:
Crusted demodicosis of the face. Primary human demodicosis showing multiple partly confluent papulopustules with thick yellowish crusts:
